
From the 1Department of Physical Medicine and Rehabilitation, Haeundae Paik Hospital, University of Inje College of Medicine, Busan, South Korea, 2Department of Neurology and Center of Clinical Neuroscience, First Faculty of Medicine, Charles University and General University Hospital, Prague, Czech Republic, 3Department of Rehabilitation Medicine, Royal Melbourne Hospital, Parkville, 4Department of Medicine (Royal Melbourne Hospital), University of Melbourne, Parkville, 5Australian Rehabilitation Research Centre, Royal Melbourne Hospital, Parkville, and 6School of Public Health and Preventive Medicine, Monash University, Victoria, Australia
Objective: To critically appraise published clinical practice guidelines (CPGs) for brain tumours, and to synthesize evidence-based recommendations from a rehabilitation perspective.
Methods: A comprehensive literature search included: health science databases, CPG clearinghouse/developer websites, and grey literature up to March 2018. All brain tumour CPGs that reported systematic methods for evidence search, and clearly defined recommendations supporting evidence for rehabilitation interventions were included. Three authors independently selected potential CPGs and assessed their methodological quality using the Appraisal of Guidelines, Research and Evaluation (AGREE-II) Instrument. Recommendations from included CPGs were categorized from a rehabilitation perspective.
Results: Of the 11 CPGs identified, only 2, developed by the National Institute for Health and Clinical Excellence (NICE) and the Australian Cancer Network (ACN), included rehabilitation components for the management of brain tumours. Both CPGs were of moderate quality. The recommendations reported were generic, and only the ACN guidelines provided detailed recommendations for rehabilitation interventions. Both guidelines recommend a comprehensive multi-disciplinary care approach. Detailed comparison, however, was not possible due to inconsistent recommendations, making it difficult to summarize rehabilitative care.
Conclusion: Despite rehabilitation being an integral component of the management of brain tumours, only a limited number of CPGs have incorporated recommendations for specific rehabilitation interventions. In order to improve clinical outcomes in this population future CPGs should incorporate rehabilitation interventions.
Key words: brain tumour; rehabilitation; clinical practice guidelines; critical appraisal.
Accepted Oct 29, 2018; Epub ahead of print Nov 28, 2018
J Rehabil Med 2019: 51: 00–00
*Correspondence address: Woo-Jin Kim, Department of Physical Medicine and Rehabilitation, Haeundae Paik Hospital, University of Inje College of Medicine, Busan, South Korea. E-mail: cyctaz@gmail.com
Brain tumours cause significant disability and morbidity. There are numerous published clinical practice guidelines (CPGs) for the management of brain tumours, and rehabilitation is recognized as an integral component of management of brain tumours. However, only limited numbers of these CPGs incorporate recommendations for specific rehabilitation interventions. To establish understanding of the issues of rehabilitation needs in brain tumours survivors, and synthesise evidence-based recommendations from rehabilitation perspective, published CPGs for brain tumours were critically appraised. Gaps in current literature were identified, and need of incorporation of rehabilitation interventions are highlighted. This is for future direction/recommendations in developing new CPGs to guide clinicians and to improve clinical outcomes in this population.
Brain tumours (BT) comprise 2% of all cancers, affecting 7 per 100,000 population annually worldwide (1). Overall incidence of BT is increasing, especially in the population over 60 years of age (2). In Australia, there are an estimated 1,400 new cases per annum, which account for 1,200 deaths annually (3). BT can have a devastating impact on patients (carers/family) and are associated with significant costs and socioeconomic implications, with increased demand for healthcare, social and vocational services (3, 4). In Australia, the estimated mean overall healthcare system cost of BT is 5 times higher than for patients with breast or prostate cancer (5).
Recent therapeutic advances have improved the survival rates of persons with BT. However, many have residual neurological deficits, leading to physical, cognitive, psychosocial and behavioural impairments, which limit everyday activity and participation (6, 7). Furthermore, many treatments for BT, such as radio-therapy, chemotherapy and surgery are associated with adverse events. Therefore, patients require integrated and coordinated long-term management, including rehabilitation, for improvements in their functional, mental and emotional state, and quality of life (QoL) (7).
Rehabilitation for survivors of BT can be challenging, as they can present with various combinations of problems, which may fluctuate, with unpredictable prognoses, and often the disease itself has a progressive nature (3, 8, 9). There is evidence to support comprehensive multidisciplinary rehabilitation for functional improvement and psychosocial adjustment (10, 11). Previous reports suggest that patients with malignant BT can make functional gains equivalent to those with stroke and traumatic brain injury in inpatient rehabilitation settings (9, 12). There remains, however, an unmet need in the BT population, as only a limited proportion of survivors receive appropriate rehabilitation intervention (13).
Clinical practice guidelines (CPGs) are systematically developed evidence-based recommendations to optimize the quality of healthcare and to guide clinicians in making appropriate decision making for improved clinical outcomes (14, 15). The worldwide published CPGs for BT vary considerably in terms of scope, developing process, search methods for evidence, strength of evidence used in formulating recommendations, etc. There is variation in the quality and consistency of recommendations amongst CPGs, as they are developed by different organizations, making it difficult for practitioners to choose the appropriate recommendations (16). Therefore, critical appraisal and evaluation of these guidelines is important (17).
To our knowledge, published BT guidelines have not been systematically and qualitatively appraised to date, especially for their recommendations regarding rehabilitation. The aims of this study are to critically appraise published CPGs for the management of BT, and to synthesize the evidence-based recommendations provided from the rehabilitation perspective in order to guide treating clinicians.
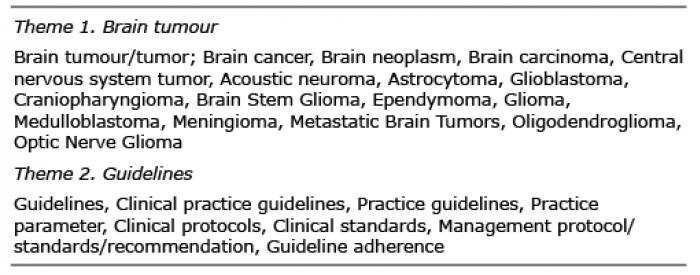
A review of the literature for published CPG on the management of persons with BT was undertaken on 21 March 2018 using a multipronged approach. A comprehensive search of the following health science databases was undertaken: Cochrane Library, PubMed, EMBASE, and CINAHL. The search strategy included combinations of multiple search terms (both MeSH and keyword text terms) for 2 themes: BT and guidelines (see Appendix 1). Various CPG clearinghouse websites and CPG developer websites were explored for potential CPGs (Table I). A search of grey literature was conducted using different internet search engines and websites: such as System for Information on Grey Literature in Europe; New York Academy of Medicine Grey Literature Collection and Google Scholar. In addition, various healthcare institutions; and governmental and non-governmental organizations associated with BT were explored. The bibliographies of identified CPGs were scrutinized, and authors and known experts in the field were contacted for further information if required.
Appendix 1. Search terms
Table I. List of organizations searched
CPGs were included if they focused on the management of BT and met the following criteria:
The scope of the CPG focused specifically on treatment of BT with systematically developed recommendations, strategies, or other information for rehabilitation.
The CPG was produced under the auspices of a relevant professional organization.
The development process included a verifiable, systematic literature search and review of existing evidence published in peer-reviewed journals (the Appraisal of Guidelines, Research and Evaluation (AGREE II) Instrument item 8); and defines an explicit link between the recommendations and supporting evidence (AGREE II Instrument item 12).
CPG developed, reviewed, or revised within the last 15 years (2003 onwards).
CPG targets adult participants (> 18 years of age).
Exclusion criteria included: CPGs focused solely on the management of other cancers; BT in the paediatric population; CPG does not include or explicitly describe the rehabilitation component; non-English publications.
Where a single CPG was reported and/or published in several different formats with varying degree of detail, only the original and latest update version with the most detailed description of its development was included.
Three authors (JK, KN, BA) independently appraised the included CPGs using the structured AGREE II Instrument developed by the AGREE collaboration (http://www.agreetrust.org/?o=1397). The AGREE II Instrument contains 23 items organized in 6 domains: scope and purpose; stakeholder involvement; rigour of development; clarity and presentation; applicability; and editorial independence. All authors independently scored each item of the instrument on a 7-point Likert scale: from 1vstrongly disagree to 7 = strongly agree. Furthermore, 2 overall appraisal items assessed the overall quality of the guidelines and whether it should be recommended for practice. Fleiss’ kappa statistic was used to determine the inter-rater reliability amongst the authors’ scores. Any disagreement or discrepancies were resolved with the fourth author (FK) and by a final group consensus. Furthermore, as aggregate scoring across domains is not recommended by the AGREE Enterprise, the AGREE II-Global Rating Scale (AGREE II-GRS) was used to rate overall quality on a 7-point scale (from 1 = lowest quality to 7 = highest quality) and categorized as: “excellent quality”= score 7/7, “high quality” = 5–6/7, “moderate quality” = 4/7 and “poor quality” = 0–3/7. The AGREE-II instrument is a validated appraisal tool for thorough quality assessment of guidelines and is widely used (18–24).
A standard pro-forma was used for data extraction from all CPGs. The form included: publication and search date, objectives/scope, methodology used, evidence-supported recommendation, and limitations. Three authors (JK, KN, BA) extracted the evidence-based recommendations, specifically for the rehabilitation, and categorized them into the following groups: (i) initial clinical assessment, (ii) observation and management, (iii) triage and discharge planning, and (iv) patient information and patient follow-up.
The searches retrieved 458 published titles and abstracts. Ten titles met the inclusion criteria and were selected for closer scrutiny. Full texts of these articles/reports were retrieved and 3 reviewers (JK, KN, BA) performed the final selection. One report that met inclusion criteria was identified from bibliographies of relevant articles. The search did not identify any specific guidelines for rehabilitation of persons with BT. Of the 11 CPGs identified, only the following 2 generic CPGs for management of BT which included different rehabilitation interventions, fulfilled the inclusion criteria for this review (Table II):
A detailed description of the included guidelines and a list of excluded guidelines are given in Table III.
Table II. Characteristics of the included clinical practice guidelines
Table III. List of excluded clinical practice guidelines
The 2 included CPGs were critiqued qualitatively using the AGREE-II tool, with a global rating score of 5 out of 7. Overall, the ACN CPG scored better than the NICE CPG (total score = 115 vs 107). All 3 authors rated the guidelines “Moderate”, indicating the need for some modification for clinical applicability. The kappa level of agreement between the authors for AGREE II assessment was 0.81. A summary of the guidelines’ assessment AGREE II scores is shown in Table IV. An overview of the quality assessment of the included CPGs for each of the 6 AGREE-II domains is set out below.
Domain 1: Scope and purpose (AGREE Items 1–3). In general, both CPGs outlined the objectives and overall aim, the specific health questions, and the target population. However, both CPGs failed to provide clear or concise information on interventions, and outcomes; and did not specifically describe the state of disease, clinical condition and exclusion criteria for the target population.
Domain 2: Stakeholder involvement (AGREE Items 4–6). Both CPGs included individuals from all relevant professional groups in the guideline development, including patient advocacy groups, community group representatives, and specific details including their roles. Although the views and preferences of the target population were stated adequately, the description of relevant target-users was not sufficiently reported in either guideline.
Domain 3: Rigour of development (AGREE Items 7–14). The strength and limitations of the body of evidence, consideration of health benefits, side-effects and risks when formulating the recommendations were not well described. There were explicit links between the recommendations and the supporting evidence in both CPGs, as well as procedures for updating the guidelines. However, NICE does not provide information on the external review process, while ACN does not report the process of reviewers’ selection.
Domain 4: Clarity of presentation (AGREE Items 15–17). Recommendations in both CPGs were specific and unambiguous, with key recommendations clearly stated. However, different options were not sufficiently described for different BT populations. The importance of the rehabilitation process was highlighted in both CPGs, but without clear recommendations concerning treatment options.
Domain 5: Applicability (AGREE Items 18–21). Both guidelines failed to describe clearly the barriers and facilitators for implementation of the CPG in practice; only a few items were mentioned vaguely. Implications of resources and associated costs were not mentioned in the ACN guidelines; however, the NICE made attempts to describe costs related to hiring specialized medical staff. Both guidelines briefly mentioned tools and advice on how to apply recommendations in clinical practice; however, reviewing and monitoring criteria were not comprehensively well-defined by either of the guidelines.
Domain 6: Editorial independence (AGREE Items 22–23). The influence of the funding body on the content of the guidelines was described clearly by both CPGs. However, the conflict of interest was not provided in the NICE guidelines.
A summary of the guidelines assessment AGREE II scores is given in Table IV.
Table IV. Ratings of the included clinical practice guidelines according to the AGREE II Instrument
Despite the recognition of rehabilitation as an integral component of management of BT survivors in both included CPGs, recommendations for specific rehabilitation interventions were described ambiguously in both. The best-evidence synthesis for various rehabilitation interventions for the management of BT provided in the included CPGs are summarized below and in Table V.
Table V. Recommendations for rehabilitation interventions in the clinical practice guidelines
Multidisciplinary rehabilitation. Both guidelines recommend a comprehensive multidisciplinary approach with individually selected goals for the longer-term management of BT. The ACN outlines rehabilitation programmes as associated with improved mobility, cognitive-communication and participation. NICE states effective and timely provision rehabilitation services in optimizing function and participation; however, without specific recommendations.
Physiotherapy (PT) and occupational therapy (OT). ACN recommends PT for patients with residual motor deficits (strength, coordination, balance) and occupational therapy for residual problems in personal care and independent activities of daily living (Level III evidence). ACN describes steroid-induced myopathy, characterized by proximal muscle weakness, as a possible negative side-effect of treatment, which can be improved with a combination of PT exercise and OT. NICE mentions that PT and OT should be involved as a part of rehabilitation team; however, without specific recommendations or evidence.
Exercise. ACN recommends aerobic and resistance training for all patients with BT to enhance muscle strength and endurance. However, no specific recommendations with regards to timing, dose and intensity are provided. ACN advocates for resistance training of unaffected muscles to compensate for impaired coordination for those with ataxia and cerebellar dysfunction. There is no description of exercise therapy in the NICE guidelines.
Neuropsychological management. ACN recommends neuropsychological assessment for behavioural changes, and organic personality change in patients with BT for cognitive deficits. It recommends that depression and anxiety can interfere with a person’s capacity to make treatment decisions and should be treated with a combination of psychotherapy and cognitive behavioural therapy, together with relaxation therapy or guided imaginary to help deal with stressful situations. The NICE guidelines recommend psychological assessment and support as an integral part of comprehensive care; however, the guidelines fail to provide any specific description or evidence.
Communication and swallowing. Speech and language therapy are offered to those with communication and/or swallowing dysfunction, for aspiration intervention and adjustments to food consistency. However, NICE only mentions involvement of a speech therapist as a part of the rehabilitation team, without specific recommendations or evidence.
Compensatory aids. Both NICE and ACN recommend immediate access to specific orthoses (ankle-foot orthoses), walking sticks or walkers, and wheelchairs for BT patients with gait impairment. Neither of the 2 CPGs provides specific recommendations and/or level of evidence.
This review comprehensively evaluates and assesses the methodological quality of the published CPGs for management of BT and summarizes recommendations for applicability from the rehabilitation perspective. Despite the challenges and complexity of delivering healthcare to BT survivors, there is well-documented evidence advocating the integral role of rehabilitation (10, 11) in restoring function, minimizing complications, reducing morbidity and improving QoL (9, 27–29). This review identifies several CPGs for the management of BT published in the last decade. However, majority focus on acute radiological, surgical and medical treatments, and rehabilitation approaches are neglected. Of the 11 published CPGs identified, only 2 provide recommendations for rehabilitation interventions. Both of these CPGs (published by NICE and ACN) describe rehabilitation approaches ambiguously and provide limited information about various rehabilitation modalities. With improved survival of patients with cancer, the role of rehabilitation must be emphasized.
The overall quality of the included 2 CPGs was “moderate”. Despite increasing evidence for rehabilitation in improved physical (6, 9, 28), psychosocial wellbeing and QoL (7, 29, 30), the included CPGs failed to incorporate and provide detailed evidence-based information on many specific rehabilitation recommendations. The overall recommendations in the NICE guidelines on rehabilitation approaches is too generic, failing to provide specific description and a supporting body of evidence behind the recommendations. Only the ACN guidelines provided a comprehensive description of recommendations for rehabilitation interventions with a supporting level of evidence. The ACN extensively described more specific and detailed recommendations on specific problems in patients with BT, justifying the level of evidence accordingly.
The key outcome measurements for evaluation of rehabilitation recommended by these 2 guidelines varied. ACN recommends the Barthel Index or Functional Independence Measure for motor function, activities of daily living, and cognitive-communication skills. The NICE guidelines did not recommend any specific assessment tools. It vaguely recommends QoL, functional status and patients/family satisfaction as patient-outcome measures.
The overall scope of the 2 included CPGs was diverse: the NICE CPG informs non-specialist readers about BT and management, whereas the ACN CPG was developed to provide information to medical practitioners and interested community members. There is considerable scope to improve the quality of both CPGs by highlighting aspects of applicability, the rigour of development, and the editorial independence. More detailed and specified implementation in practice and monitoring criteria should be considered in future CPGs. Evidence-based best-practice guidelines specific to BT rehabilitation should be developed further and incorporated into routine management programmes for patients with BT.
In recent years, therapeutic advances have prolonged survival rates in BT (6, 22). Despite these advances, there are often residual concerns in the post-acute and longer-term phases (24) (regarding physical, cognitive, behavioural and psychosocial problems) (6, 8, 23). These can have a cumulative effect over time and cause considerable distress to the cancer survivor, their families, and reduce QoL (24). Furthermore, treatment regimens are associated with adverse effects (4, 31) and the disease course itself can alter outcomes due to a combination of physical, cognitive, and communication deficits. There is evidence to support interdisciplinary rehabilitation for improved functional independence, mental and emotional state, QoL and participation (7). Furthermore, inpatient rehabilitation can result in functional improvement and going-home rates are on par with individuals with stroke or traumatic brain injury (7). Studies have shown that participation in multidisciplinary rehabilitation, significantly improved function (27, 32–35), with some gains in BT survivors maintained for up to 6 months (10).
The AGREE-II Instrument is a useful tool used worldwide for evaluating the quality of guidelines. However, it has some limitations; especially regarding the assignment of scores, as there are no clear definitions for different scores (36). Hence, at times scoring may be influenced by subjectivity (37). Nonetheless, the AGREE-II Instrument remains the most widely accepted method and validated tool available for this purpose. A clinimetric appraisal of the AGREE II tool was beyond the scope of this review. The AGREE-II tool focuses on methodological issues related to the guideline development process and reporting, and which is explicitly insufficient to ensure that recommendations are valid and appropriate (36, 37). The tool itself cannot appraise the quality of evidence supporting the recommendations. This is clearly reflected in the findings of this review, with included CPGs applying multiple sources for generating the evidence underlying the recommendations. The authors employed 3 reviewers per guideline for the critical appraisal, with input from others in case of discordance, and extensive consultations with experts in the field to minimize these shortfalls. Despite multiple attempts, we did not receive a comprehensive report on the methodological CPG development process from the guideline developers. Therefore, the raters’ judgement was based explicitly on the information stated in the guidelines and/or information obtained from developers’ websites.
Some limitations of this study in terms of methodology and completeness of the literature retrieval and review process cannot be ruled out. First, since only published CPGs in the specific searched health-science databases and guideline-publishing organizations were searched, there is a possibility that relevant CPGs from other sources may have been missed. Nevertheless, our comprehensive systematic search strategy of prominent databases in the medical literature and grey literature and search of prominent CPG developing organizations; and manual screening of bibliographies, mean that it is unlikely that any important CPGs were missed. Furthermore, only guidelines published in English language were retrieved, therefore there is a likelihood of CPGs published in other languages being missed. However, a comprehensive search of guidelines clearinghouses was conducted, which includes information on all published guidelines without language restriction. This review included only adult populations with BT; the paediatric BT population was beyond the scope of the review and expertise of the research team. Interestingly, the majority of published CPGs on BT were generally more attentive to the medical, surgical and radiological treatments, and only 2 CPGs included information on rehabilitation approaches. The underlying evidence for the recommendations in both of the included CPGs (NICE and ACN) appears outdated and old (> 10 years) (update of the NICE guidelines is currently in progress; personal communication with the developers). To our knowledge, a large body of evidence (clinical trials, systematic reviews) is now available since the development of these 2 CPGs. Examination of this evidence will be critical in formulating the recommendations in future updates or development of new CPGs in this area.
BT have a significant effect on both survivors and their caregivers/family (5). In the community patients are often confronted by new care demands, personal relationship, financial constraints, relationship stress, relapse, recurrence, etc., requiring integrated multidisciplinary care, including rehabilitation (38). However, there is lack of awareness about the integral role of rehabilitation amongst many healthcare professionals, as surgical, medical, and radiological treatments are considered a priority. The aim of BT rehabilitation is not only management of disability and/or minimizing symptoms and treatment-related complication effects, but also enhancing participation. Interventions such as physical therapy, psychological interventions (psychotherapy, cognitive behaviour training) and others can reduce disability, and improve participation.
This review was unable to synthesize rehabilitation-related recommendations sufficiently from the publi-shed CPGs, due to the limited numbers of BT CPGs with rehabilitation management, and the inconsistency in reporting underlying evidence to support these recommendations. The 2 included CPGs (NICE and ACN), were moderate in quality, and the overall recommendations formulated were generic. This resulted in difficulty in comparing and summarizing recommendations for rehabilitation approaches. However, both CPGs recommend comprehensive assessment of functional limitations and the various levels of disability in this population at regular intervals in order to establish a better care model and to optimize physical independence and participation (12).
Despite evidence to support rehabilitation interventions in patients with BT (2, 11), literature evaluating rehabilitation interventions is scarce (2, 11). There is lack of robust studies evaluating the effectiveness of many rehabilitation interventions. The findings from this review highlight the need for systematic data collection in clinical practice and research into the course of BT, including long-term follow-up outcomes. Although randomized controlled trials (RCTs) are considered the “gold standard” for high-level evidence, they are less appropriate in studying rehabilitation interventions. Patients’ (and/or caregivers’) perspective must be incorporated into rehabilitation programmes. Outcome measures should reflect activity and restriction in participation. There is a need for a suitable battery of measures to capture change in physical ability, symptoms and longer-term outcomes relating to psychosocial adjustment and QoL.
This study reviews CPGs for the management of persons with BT from the rehabilitation perspective. Delivery of rehabilitation interventions in patients with BT should not differ from other neurological conditions, such as stroke or traumatic brain injury; however, owing to the disease characteristics, rehabilitation is often overlooked in this patient cohort. Current CPGs for the management of BT do not provide consistent and detailed information on rehabilitation management; thus it is challenging to synthesize recommendations for rehabilitation approaches specific to BT survivors. Both of the guidelines included in this review provide generic recommendations regarding rehabilitation modalities. Developers of future CPGs should comprehensively evaluate and incorporate rehabilitation modalities in the management of patients with BT, so that these interventions can be integrated into routine clinical practice in order to improve patient outcomes.


 Click to show fullsize
Click to show fullsize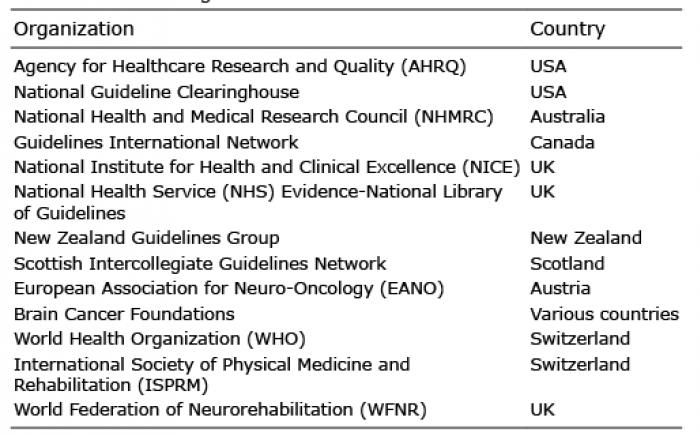 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize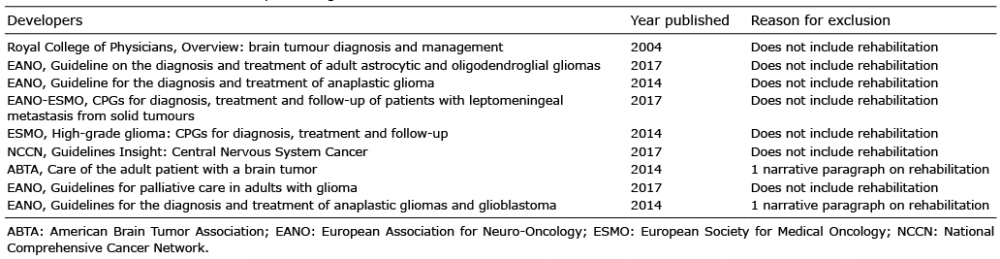 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize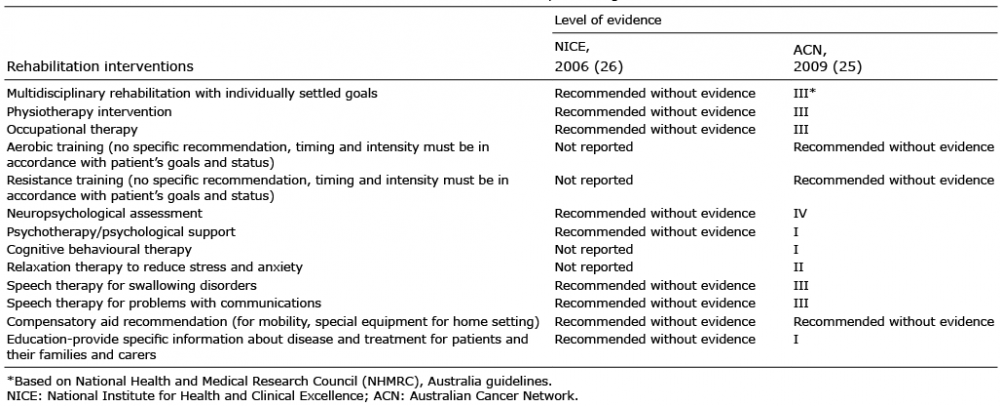 Click to show fullsize
Click to show fullsize